A needle biopsy is a common technique for diagnosing lumps in the head and neck region. The procedure is formally called fine needle aspiration (FNA) and involves pulling cells into a small needle for analysis. Below, I have answered common questions about the procedure to help you become a more informed patient and to hopefully remove some of the anxiety from the experience.
What is a needle biopsy procedure and why might you need one?
A lump felt by a patient or his or her doctor or an abnormal nodule/lump/mass seen on an imaging test (CT scan, MRI, etc.) may prompt the need for a biopsy. Rather than a big surgery to remove the lump, a needle biopsy can be done easily in the office (with the patient awake). Depending on the biopsy results, the appropriate treatment plan can be determined.
What should I expect during the needle biopsy?
Needle biopsy is performed in the office with the patient awake and relaxed in a reclined exam chair.
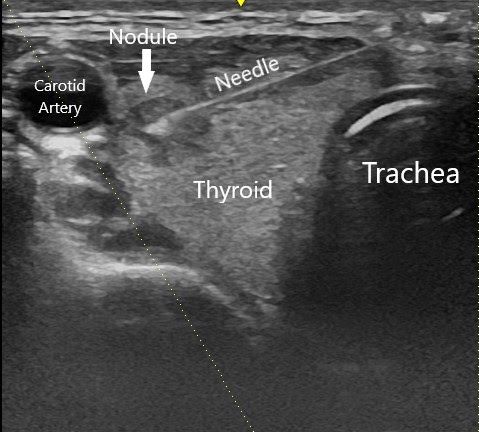
Often an ultrasound probe is used to determine the location of the mass and to guide the needle safely into the mass while avoiding the nearby blood vessels (the needle shows up on the ultrasound in real-time!). Using ultrasound is particularly important when the mass cannot be felt easily. Use of ultrasound increases safety as well as accuracy[i].
The patient can leave the office right after the biopsy is performed and is able to return to normal activities the same day. A driver or escort home is not required.
Is needle biopsy painful?
Most patients are pleasantly surprised by the ease of the procedure and minimal amount of pain that they experience. Different physicians use different techniques which can result in different levels of comfort for the patient. I typically use local anesthetic which makes the procedure completely painless after placement of the anesthesia. I also prefer to use small gauge needles (25 gauge) which further decreases the amount of discomfort. There is typically no bleeding or bruising after the procedure. A small amount of soreness is sometimes felt in the area of the biopsy for a few days following the procedure and can be managed with over the counter pain medications.
What are the potential results of a needle biopsy?
Imagine a car in a closed garage. The car in this example represents the mass within the body. If you were standing outside of the closed garage, you would not be able to tell what kind of car is inside. If someone were to go inside the garage and randomly remove a handful of parts from the car and bring them to a car expert, that expert could try to work backwards and attempt to figure out the type of car. If the expert was brought a Mercedes hood ornament it would be quite easy to tell the make of the car. On the other hand, if they were brought only a large tire, they would probably infer the car is a truck or SUV, but not be able to say much beyond that.
Analysis of FNA samples is similar in that the pathologist is only able to see a “part of the whole,” but thankfully they are usually able to make a diagnosis. Occasionally, the diagnosis is unclear, regardless of the skill of the pathologist, and there is also a small chance of a wrong diagnosis.
These limitations aside, a needle biopsy is much faster and safer than a surgical biopsy done in the operating room and usually produces useful information about the diagnosis to guide treatments.
Results of a fine needle aspiration generally fall into one of the following categories:
- Non-diagnostic – This generally means that not enough cellular material was obtained and therefore the pathologist cannot make a determination as to the identity of the tissue.
- Benign – Sufficient material was obtained, and it all looks normal
- Suspicious/Atypical – Some or all of the cells obtained have abnormal features, but they are not specific enough to make a definitive diagnosis
- Benign Neoplasm – The cells are abnormal, but not cancerous
- Cancer
Specific FNA classification systems for head and neck
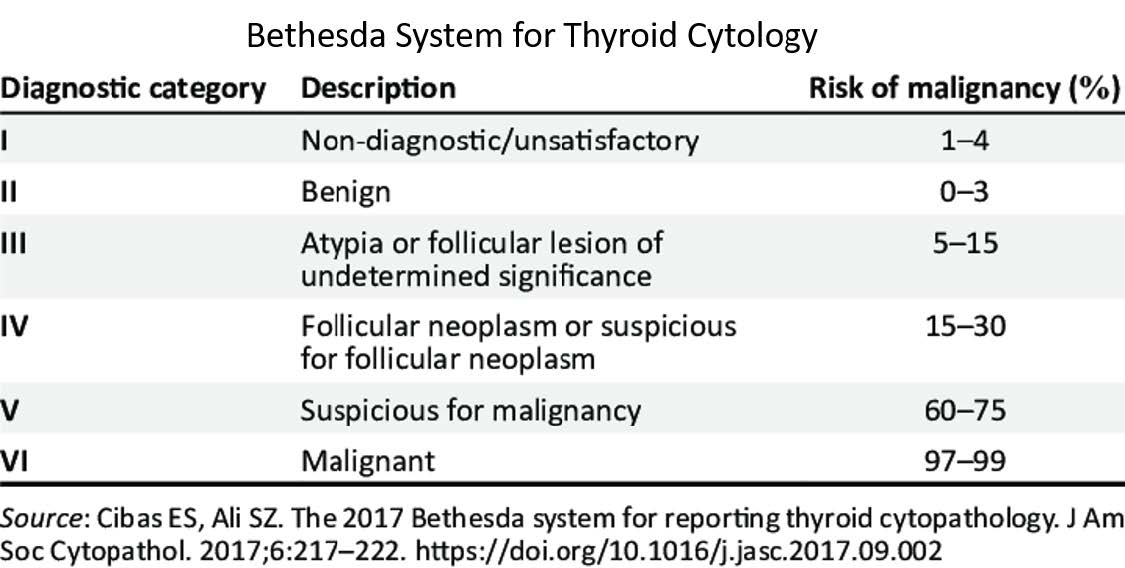
There are specific FNA classifications for certain parts of the head and neck. The two most common are the Bethesda System for thyroid and the Milan System for salivary tissue.
What is flow cytometry?
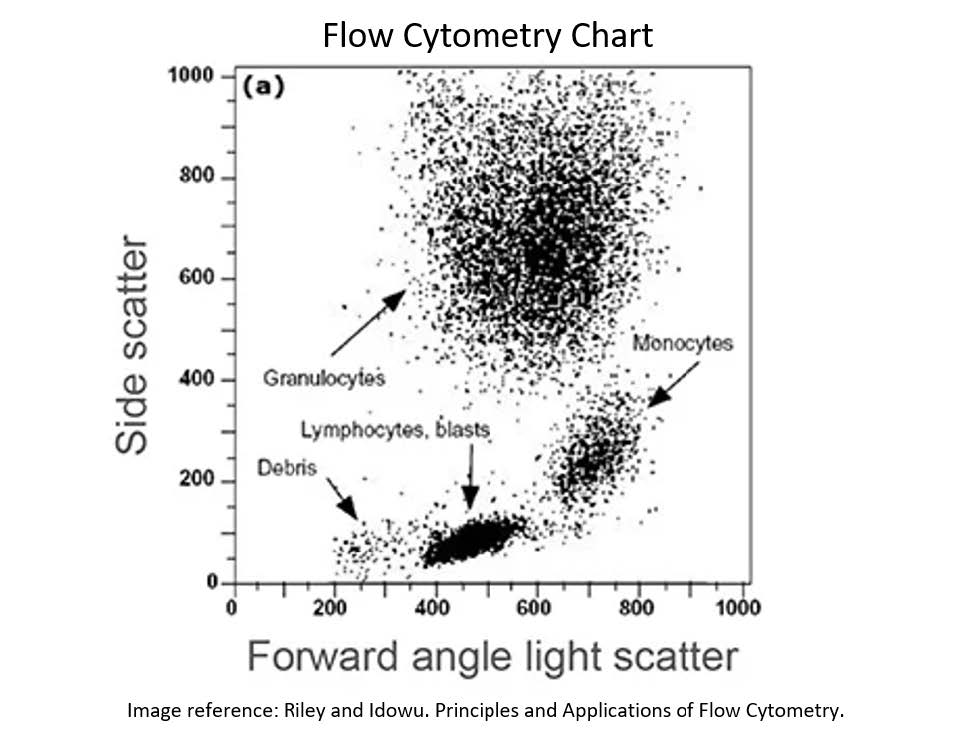
Flow cytometry is a method of analyzing FNA samples to rule out a cancer of the lymph node cells called lymphoma. A flow cytometry sample is collected in the same way as a regular needle biopsy sample.
A normal lymph node contains a variety of different types of cells called lymphocytes. Cancer of the lymphocytes (lymphoma) can develop when one of these cells takes over and grows uncontrollably. When a flow cytometry sample is analyzed, the lymphocytes are sorted by type and counted. If there is a predominance of one type of cell, this raises the suspicion for lymphoma. A normal flow cytometry result significantly decreases the possibility of lymphoma, but there are certain lymphoma types (some large cell types and Hodgkin’s lymphoma) which might not be detected on flow cytometry.
What is a core biopsy?
A core biopsy is a needle biopsy that is performed with a slightly larger needle. The increased needle diameter allows a “core” of tissue to be extracted for analysis. Rather than a sample of separate, free-floating cells, the pathologist can see the relationship between cells which increases the ability to make a diagnosis. A core biopsy is typically performed after a non-diagnostic or inconclusive fine needle aspiration.
Does FNA lead to spread of tumor cells?
Fine needle aspiration is the standard of care for diagnosis of malignant lymph nodes and the medical evidence supports its safety. However, there is often still concern about tumor cells being seeded along the path of the needle and there have been some reported cases of this happening, especially with larger needle sizes. The risk of tumor seeding in head and neck biopsies is estimated to be about 0.00012% (about 1 in 830,000 biopsies)[ii] . This very low risk is outweighed by the significant benefits of the information gained from needle biopsy.
References:
[i] Izquierdo R, Arekat MR, Knudson PE, Kartun KF, Khurana K, Kort K, Numann PJ. Comparison of palpation-guided versus ultrasound-guided fine-needle aspiration biopsies of thyroid nodules in an outpatient endocrinology practice. Endocr Pract. 2006 Nov-Dec;12(6):609-14.
[ii] Shah KS, Ethunandan M. Tumour seeding after fine-needle aspiration and core biopsy of the head and neck--a systematic review. Br J Oral Maxillofac Surg. 2016 Apr;54(3):260-5
Find an ENT & Allergy Associates Doctor Near You, or Explore More Blog Topics